Introduction: The Evolution of the Maxillofacial Scope
The contemporary practice of oral and maxillofacial surgery (OMS) has undergone a profound transformation, shifting from a focus on localized dentoalveolar procedures to a comprehensive “Total Face” approach. This expansion was professionally anchored by the American Dental Association’s (ADA) decision to redefine the scope of dentistry, moving beyond “teeth and supporting structures” to encompass the entire maxillofacial complex and its associated anatomical regions.
Orthognathic surgery represents the pinnacle of skeletal repositioning, addressing malocclusions and facial disproportions that are beyond the reach of traditional orthodontics alone. While orthodontics manages dental alignment, orthognathic surgery targets the “skeletal base”.
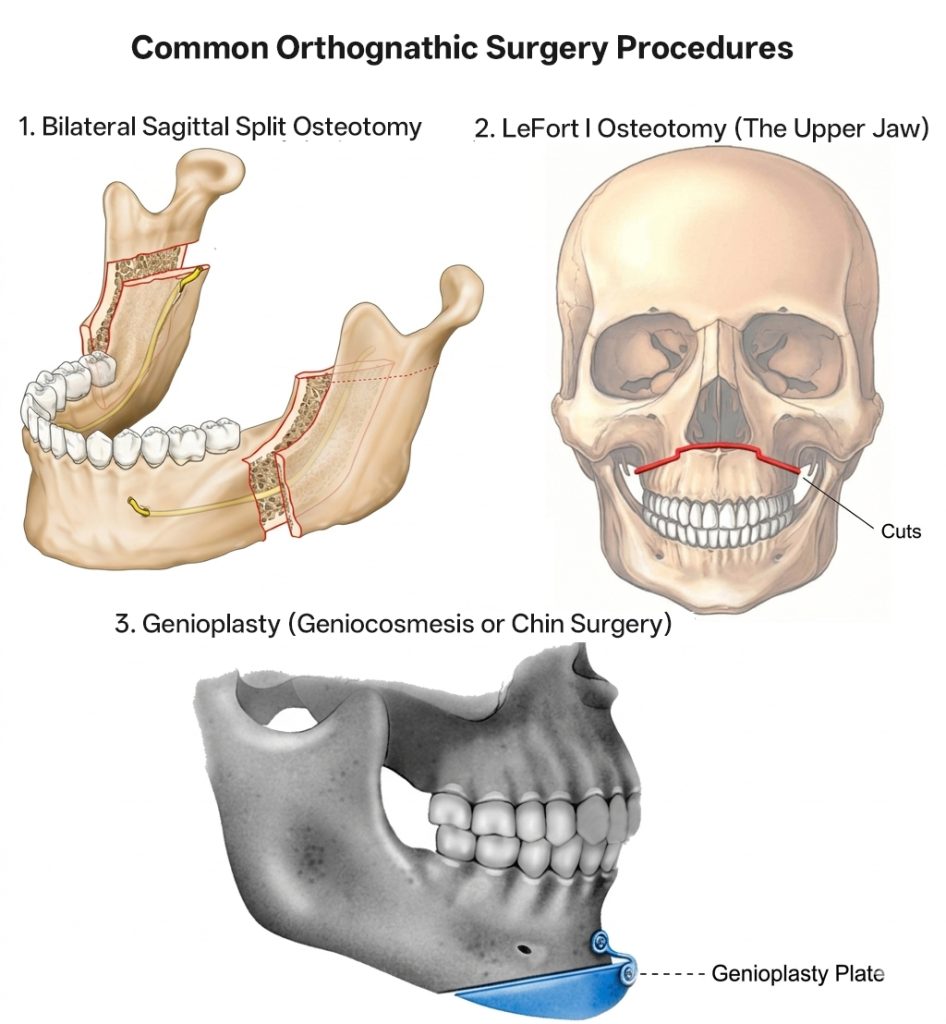
1. LeFort I Osteotomy (The Upper Jaw)
Commonly referred to as a “maxillary advancement” or “setback,” the LeFort I osteotomy allows for the movement of the maxilla in all three planes of space. It is the primary solution for:
- Vertical Maxillary Excess: Correcting the “gummy smile” by superiorly repositioning the bone.
- Midface Deficiency: Enhancing facial projection in patients with a concave profile.
2. Bilateral Sagittal Split Osteotomy (BSSO – The Lower Jaw)
The BSSO is the workhorse of mandibular surgery. It allows the surgeon to slide the lower jaw forward to correct retrognathism or backward to address skeletal underbites. The complexity of BSSO lies in protecting the inferior alveolar nerve while achieving a stable bony interface for healing.
3. Genioplasty (Geniocosmesis or Chin Surgery)
Often performed as an adjunctive procedure, genioplasty involves the surgical repositioning of the chin. Research indicates that genioplasty is among the most frequently performed cosmetic procedures in OMS residencies, reflecting its critical role in balancing the facial profile.
As a result, facial cosmetic and reconstructive surgery is now a mandated core pillar of OMS residency training. To meet the standards set by accreditation bodies like the Commission on Dental Accreditation (CODA), surgeons must achieve proficiency in both the functional reconstruction and aesthetic enhancement of the face, jaw, and neck.
Global Trends: The Shift Toward Digital Precision
The global landscape of orthognathic surgery is currently defined by a “digital revolution” that has moved surgical planning from 2D cephalometric tracings to 3D virtual environments.
- Virtual Surgical Planning (VSP): Utilizing high-resolution CT and MRI scans, surgeons can now create a 3D radiographic display of a patient’s internal anatomy. This allows for the precise manipulation of bony segments on a computer before the first incision is made.
- 3D-Printed Surgical Guides: In advanced clinical centers across Europe, North America, and Asia, the use of patient-specific 3D-printed templates is becoming standard. These guides transfer the digital plan to the operating room with sub-millimeter accuracy, ensuring that osteotomy lines are precisely where the data dictates.
- Intraoperative Navigation: Pilot programs are now utilizing navigational systems linked to complex 3D images, providing surgeons with a “head-up display” during the operation. This technology functions as a GPS for the face, allowing for real-time tracking of surgical instruments relative to critical nerves and vascular structures.
Clinical Indications: Function, Aesthetics, and Beyond
The expansion of orthognathic surgery is driven by a combination of an aging population, increased aesthetic awareness, and the recognition of the jaw’s role in systemic health.
- Obstructive Sleep Apnea (OSA): Maxillomandibular advancement (MMA) has emerged as one of the most effective surgical treatments for OSA, physically expanding the pharyngeal airway by moving the skeletal framework forward.
- Temporomandibular Joint (TMJ) Health: By correcting skeletal malalignments, surgeons can often alleviate the chronic pain and joint degeneration associated with long-term malocclusion.
- Age-Related Skeletal Changes: As the global population ages, there is an increased focus on how skeletal support affects the sagging of soft tissue. Corrective surgery can provide the structural “scaffolding” required for more enduring cosmetic results.
The Challenge of Soft Tissue Mastery and Residency Training
Despite the precision of 3D planning, the ultimate challenge remains the “Soft Tissue Envelope”. The face is a complex, three-dimensional maze where blood vessels and nerves reside at varying depths.
Research published via PubMed (ID: 30921155) highlights the intensity of OMS training. Accredited residency programs often complete an average of 211 facial cosmetic procedures over a 5-year period. This high volume of cases—which includes rhinoplasty, blepharoplasty, and facelifts in addition to skeletal surgery—ensures that graduating surgeons have the “Total Face” perspective required for modern aesthetics.
A critical finding in these studies is that 4-year OMS certificate programs and 6-year dual-degree (MD/DDS) programs both provide robust experience, often exceeding the minimum graduation requirements of other medical specialties commonly associated with facial plastics.
Conclusion
In summary, the distinction between traditional orthodontics and orthognathic surgery lies in the boundary between dental alignment and skeletal structure. While orthodontics manages the position of the teeth, orthognathic surgery addresses the very foundation upon which those teeth reside. For patients with complex skeletal malocclusions, surgery is not merely an elective aesthetic choice but a functional necessity that orthodontics alone cannot fulfill.
The global landscape of orthognathic practice is currently defined by the shift toward high-precision procedures—such as LeFort I and BSSO—supported by a robust digital workflow. From virtual surgical planning (VSP) to 3D-printed guides, the integration of technology has significantly reduced intraoperative risks and improved predictable outcomes. However, the field continues to face the enduring challenge of the “soft tissue envelope,” where the biomechanical response of skin and muscle remains a complex variable that requires both surgical intuition and extensive clinical experience.
As Oral and Maxillofacial Surgeons continue to bridge the gap between functional reconstruction and facial plastics, the synergy of skeletal mastery and digital innovation will remain the gold standard. The future of the specialty lies in this “inside-out” approach, ensuring that every structural change is rooted in anatomical precision, long-term stability, and the pursuit of both functional and aesthetic excellence.
References
- Stranix, J. T., et al. (2019). “Facial Cosmetic Surgery Training in American Oral and Maxillofacial Surgery Residencies: A 5-Year Analysis.” Journal of Oral and Maxillofacial Surgery. [PubMed ID: 30921155].
- Posnick, J. C. (2022). Orthognathic Surgery: Principles and Practice. 2nd Edition. Elsevier.
- Zheng, G. S., et al. (2021). “The Role of 3D Printing and Virtual Surgical Planning in Orthognathic Surgery: A Global Perspective.” International Journal of Oral and Maxillofacial Surgery.
- American Dental Association (ADA). (2023). “Policy on the Definition of Dentistry and the Scope of Oral and Maxillofacial Surgery.”
- Mehra, P., & Wolford, L. M. (2020). “Long-term Stability of Bimaxillary Orthognathic Surgery: A Systematic Review.” Journal of Stomatology, Oral and Maxillofacial Surger